颞部三角形脱发-读书报告6
2017年11月20日 12925人阅读 返回文章列表
Keywords: growth (anagen, 生长期), cessation (catagen,退行期), and rest (telogen,休止期) phases.
Temporal triangular alopecia
颞部三角形脱发
Clinical features
临床特征
Temporal triangular alopecia (congenitaltriangular alopecia, Brauer nevus)1
was described by Saboreau in 1905.2 It usually appears in the early years of
life rather than at birth.3,4 Familial cases rarely occur.5 Occasionally, the disease
presents in adults.6,7
颞部三角形脱发(先天性三角形脱发,Brauer痣),由Saboreau在1905年报道。它通常出现在生后的几年,而不是在出生时。家族性的病例罕见发生。偶见于成年人。
It involves one sideof the scalp and characteristically presents as a single
patch of alopecia withits base directed towards the frontotemporal area (Fig.
22.54).8 Occasionally, other areas are affected and, exceptionally, patients
show bilateral involvement.7 Clinical examination reveals vellus hairs in the
almost complete absence of terminal hairs andinflammatory changes (Fig.
22.55).
本病仅累及一侧头皮,特征性表现为单一的三角形脱发斑,其底边朝向额颞区(Fig.22.54)。偶尔其它区域也可受累,极罕见的情况下出现两侧受累。临床检查发现局部毳毛,终毛几乎完全消失和炎症改变(Fig.22.55)。

Fig. 22.54
Triangularalopecia: note the characteristic triangular patch of alopecia.
三角形脱发:注意特征性的三角形脱发斑。

Fig. 22.55
Triangularalopecia: in this close up view inflammatory changes are absent.
三角形脱发:在这个近视图特写中可看到炎性改变缺如。
Temporal triangular alopecia has been describedin association with
aplasia cutis, phakomatosis pigmentovascularis,mental retardation, epilepsy,
leopard syndrome, and congenital heart diseasewith renal and genital
abnormalities.9–13
有报告颞部颞部三角形脱发和皮肤发育不良、色素血管性斑痣性错构瘤、智力低下、癫痫、豹皮综合征、先天性心脏病伴肾脏和生殖器畸形有关。
Pathogenesis and histological features
发病机制和组织学特征
The genetic basis of the disease is uncertain buta dominant trait has been
suggested.14
本病的遗传基础尚不清楚,有人提出为副显性特征。
The epidermis and dermis are normal, but thereare almost no terminal hairs
and the number of vellus hairs is increased. Thesebaceous and eccrine glands
are normal. Fibrous stellae and inflammation areabsent (Fig. 22.56). In general,
the histological appearanceis very similar to that of a normal skin biopsy.
表皮和真皮正常,毳毛的数量增加,但几乎没有终毛。皮脂腺和小汗腺正常。没有纤维索和炎症(Fig.22.56)。总之,这个疾病的组织学表现和正常的皮肤活检非常相似。
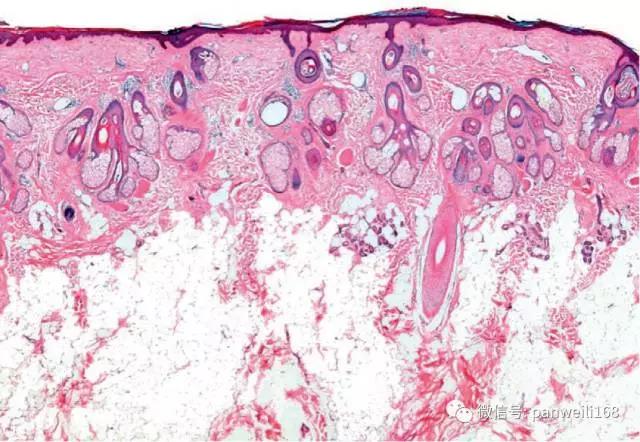
Fig. 22.56
Triangularalopecia: this biopsy is taken from the edge of a lesion. One terminal hairfollicle is present on the right side of the field (unaffected scalp).Miniaturized vellus hairs are seen in the left half (affected scalp). There areno stellae or inflammatory cells.
三角形脱发:活检取自皮损的边缘。在视野的右侧有一个终毛的毛囊(非受累的头皮)。微小化的毳毛可在视野的左侧看到(受累处头皮)。没有纤维索或炎症细胞。
Differential diagnosis 鉴别诊断
The differential diagnosis includes other causes of circumscribed non-scarringalopecia, particularly alopecia areata and tinea capitis. In the former
the bulbs of anagen follicles are surrounded and infiltrated by lymphocyte
and in the latter the microscopic findings of fungal organisms by hydroxide
potassium (KOH) or PA S and/or culture of the hair shaft are sufficient to
establish a diagnosis.
鉴别诊断包括其他原因引起的非瘢痕形成性脱发,尤其是斑秃和头癣。在前者的生长期毛囊周围浸润有淋巴细胞,而后者在显微镜下可看到真菌的产物,通过氢氧化钾(KOH)或PAS染色,和或发干培养,上面这些检查足以来确立诊断。
(颞部三角形脱发文章完)
本文译文:浙江省人民医院樊莎莎医师 2017-11-10
 浙公网安备
33010902000463号
浙公网安备
33010902000463号