皮肤病理英文晨读报告(1)
2017年11月14日 9210人阅读 返回文章列表

图中右一为皇幼明大夫
每周的工作日早上7:00~8:00,浙江省人民医院皮肤科都要进行英文专著早都会。目前在读的英文专著是《McKee's Pathology of the skin, 第四版》。从今天开始,我们每天都将发布英文专著学习报告。
CLASSIFICATION OF ALOPECIA
Classification of alopecia is often difficult, both from a clinical perspec- tive and in terms of etiology. Commonly, the cause cannot be identified and there is considerable clinical and histological overlap in the different types of alopecia. Many classifications have been proposed and the most widely accepted divides alopecia into those that are patterned and those that dif- fusely involved the scalp and into cicatricial and noncicatricial (scarring and nonscarring) variants. Nonscarring alopecia is reversible whereas cicatricial alopecia is permanent. The follicular loss in the latter may result from the scarring process or develop independently.
The main problem with this classification is that there is a great degree of overlap and clear-cut distinction is frequently not possible. In addition, some variants of alopecia (e.g., alopecia areata, trichotillomania, and traction alo- pecia) are initially nonscarring but may become scarring with time.
Scarring alopecias are classified into primary and secondary variants. Primary scarring alopecias are those in which the hair follicle is principally involved, as occurs in lichen planopilaris and lupus erythematosus. In the other variants, the hair follicle is not the main target of the inflammatory process and is destroyed as a secondary phenomenon. Examples of the latter include physical causes such as irradiation, infiltration of the scalp by tumor, inflammatory diseases including morphea, and infectious processes as may occur with fungi.1–3
Clinical features
Androgenetic alopecia is also known as common baldness and male and female pattern hair loss.1 It is caused by androgens in genetically suscepti- ble men. Typically, there is progressive miniaturization of hairs in the scalp between the ages of 12 and 40 years.
Androgens are the main regulator of normal human hair growth. After puberty, they promote transformation of vellus hair follicles into large pig- mented terminal hairs. However, androgens may also reverse this process, resulting in the gradual replacement of terminal hairs with vellus hairs and the onset of androgenetic alopecia.
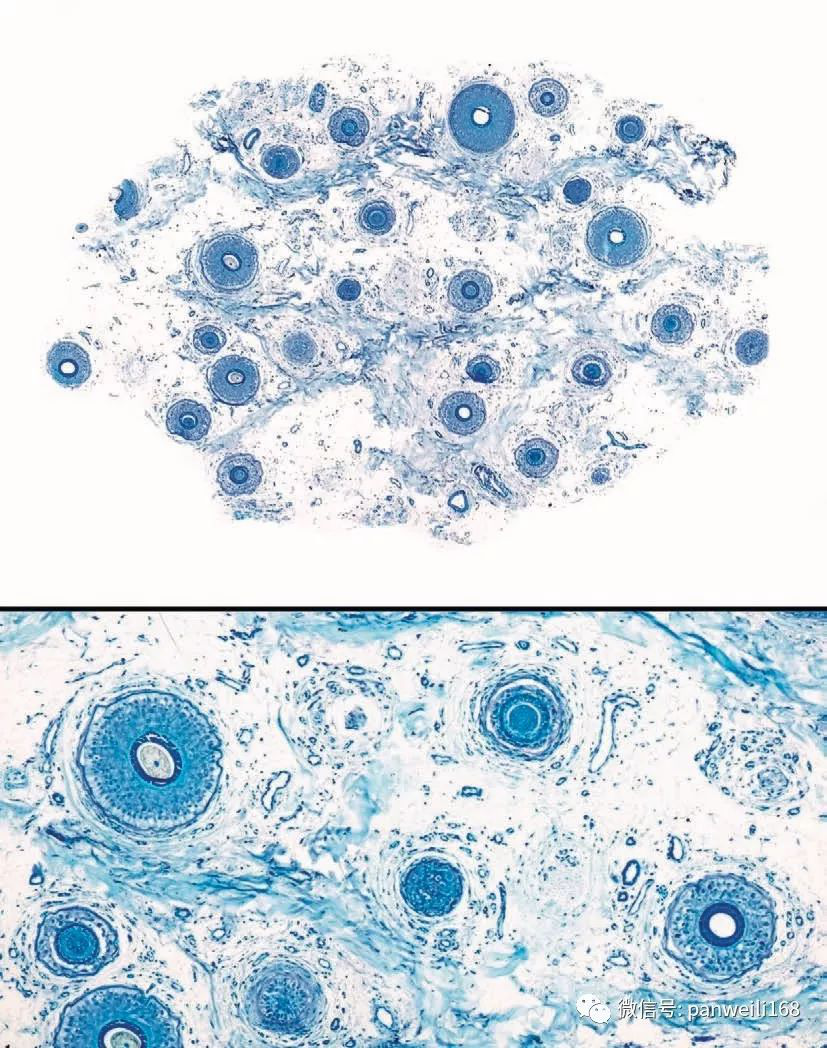
图片说明:甲苯胺蓝染色。随着脱发的进展,毛囊逐渐缩小,密度也越来越稀疏。
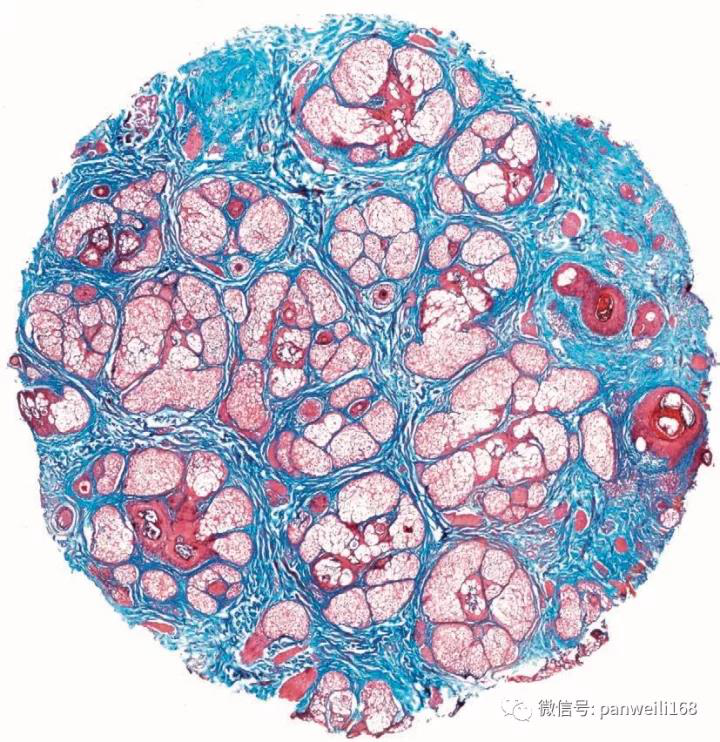
图片说明:几乎所有的毛囊都变得很小,皮脂腺凸起明显。(马松三色染色)

图片说明:毛囊单位,萎缩过程完全,但是终末期毛囊缺乏。
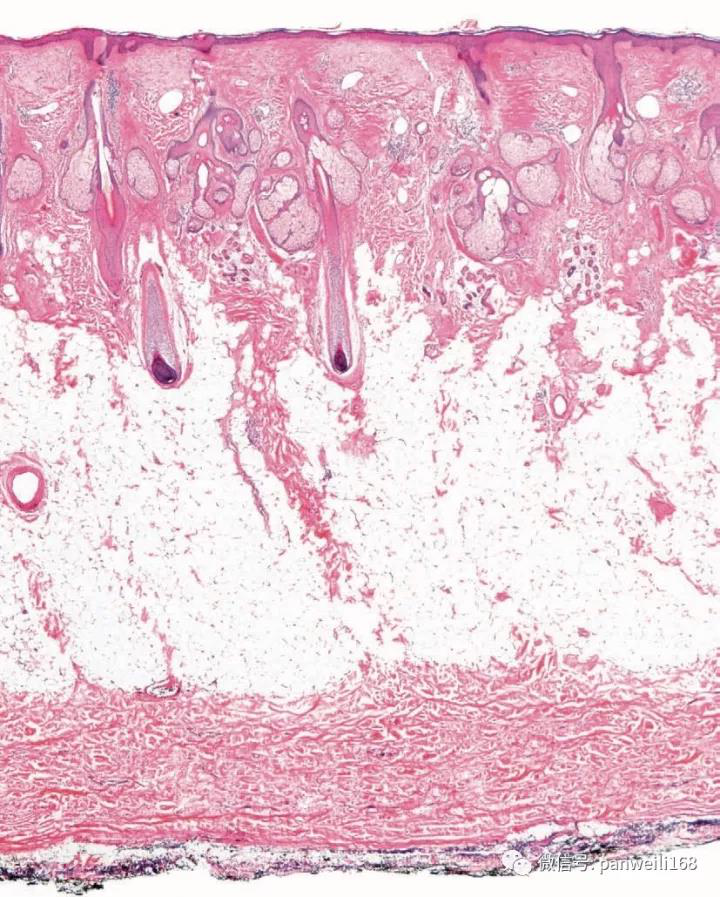
图片说明:垂直切面,只有2个毛囊进入到皮下脂肪层,其余在真皮中层都逐渐萎缩变小了。
(译者说明,如果要做头皮毛发病理切边,最好是横切和竖切组合)
脱发的分类
————————————————————
无论从临床表现还是从病因方面对脱发进行分类都存在一定的难度。病因常常难以确定,并且不同类型的脱发在临床和组织学表现上有相当的重叠。现有多种分类方法,但应用最普遍的是将脱发分为瘢痕性和非瘢痕性脱发。非瘢痕性脱发是可逆的,而瘢痕性脱发是永久的。后者毛囊的缺失可能是由瘢痕形成过程导致的或独立发展而成。这种分类方法的主要问题是有很大程度的重叠,常常难以区分。
有些脱发开始时是非瘢痕性脱发,而随着时间的延长可变成瘢痕性的,如斑秃,拔毛癖和牵拉性脱发。瘢痕性脱发分为原发性和继发性。原发性瘢痕性脱发是指那些主要累及毛囊性的疾病,如毛发扁平苔藓和红斑狼疮。在继发性瘢痕性脱发中,毛囊不是炎症过程的主要靶部位,而是继发性地被破坏,包括物理原因如放射,头皮被肿瘤浸润,硬斑病等炎症性疾病和真菌感染等感染性疾病。
非瘢痕性脱发
—————————————————
雄激素源性脱发
———————
临床特点
雄激素源性脱发:雄激素源性脱发多(普通脱发、遗传性头发稀少)发生在有遗传背景的男性中,是雄激素依赖性的。以22-40岁期间头发进行性减少为典型表现。雄激素是调节人类毛发正常生长的主要因素。青春期后,促进毳毛毛囊转化,或成为细的无色素毛发,或成为粗大的色素性终毛。然而,雄激素性还可逆转这个过程,使终毛逐渐被毳毛所替代,发生雄激素源性脱发。
(未完待续)
 浙公网安备
33010902000463号
浙公网安备
33010902000463号